![]()
![]()
Sameer Al-MaisaryI; Jamila KremerI; Gabrielle RomanoI; Matthias KarckI; Raffaele De SimoneI
DOI: 10.21470/1678-9741-2022-0361
ABSTRACT
Introduction: Laser lead extraction is a well-established method for removing unwanted leads with low morbidity and mortality. In this small series of cases, we documented our experience with venous thrombosis after laser lead extraction.AVB = Atrioventricular block
CAD = Coronary artery disease
CIED = Cardiac implantable electronic devices
DM = Diabetes mellitus
HTN = Arterial hypertension
LBBB = Left bundle branch block
LLE = Laser lead extraction
LV = Left ventricular
RA = Right atrial
RV = Right ventricular
SSS = Sick sinus syndrome
VT = Ventricular tachycardia
INTRODUCTION
The implantation of cardiac implantable electronic devices (CIED) is a common procedure due to increasing indications for its use to improve survival and the quality of life in patients with cardiac rhythm disorders[1,2]. Proportional to this increase there is also an increase in the complications related to those devices, like infections and dysfunction, which makes its removal a necessity[3-6]. Many techniques were developed for lead extraction but most of them were ineffective especially in removing very old leads[3,4,7]. The introduction of laser lead extraction gave the doctors a good tool for lead extraction, which has a high success rate and a relatively low risk profile[8-11]. However, this low risk profile includes some serious complications that may alter the whole prognosis of a patient after laser lead extraction. Axillo-subclavian vein thrombosis is a rare illness. To the best of our knowledge, its association with laser lead extraction was not reported until now in the literature. The aim of this study is to turn the light on some of the cases in our cohort who had suffered from symptomatic deep vein thrombosis after laser lead extraction.
METHODS
All patients who underwent laser lead extraction at Heidelberg University Hospital (Heidelberg, Germany), from May 2010 to July 2021, were retrospectively investigated. We screened the records to identify patients who suffered from axillo-subclavian thrombosis as postoperative complication of laser lead extraction. We gathered demographic, preoperative, intraoperative, and postoperative data of the affected subjects. The diagnosis of axillo-subclavian vein thrombosis was based on clinical symptoms, physical examination, and imaging tests.
Patients were referred from external hospitals or from our electrophysiological outpatient clinic. Indications for lead extraction were pocket infection, device-related endocarditis, pain, and abandoned or non-functioning leads at the time. Pocket infection was defined as redness with or without purulent discharge from the device pocket or device erosion which may be accompanied by pain. Device-related endocarditis was defined as persistent bacteremia or sepsis in the absence of another identifiable source or the presence of vegetations on the leads or valves. Pain related to CIED or leads was considered also as an indication for extraction. Extraction of abandoned or non-functioning leads is performed if they produce obstruction to a venous system or if a new lead implantation will increase the burden of the total lead number. The use of laser sheath was indicated if the removal of the leads under simple traction was not successful. All procedures were performed under general anesthesia with continuous arterial blood pressure monitoring. Under fluoroscopic guidance, the lead extraction starts by inserting a lead locking stylet into the inner coil lumen, then a suture is tied around the insulation and the locking stylet. After that, the laser sheath (GlideLight™ 80 Hz, 14 or 16 French) was advanced over the lead until the locking stylet emerged from the other side of the laser sheath. Laser was then applied while gradually advancing the sheath over the lead under traction until the lead was freed. Transesophageal echocardiography was used to monitor the procedure. In patients with local or systemic infection, no device would be implanted unless the patient is pacemaker dependent. In that case, an epicardial pacemaker lead is implanted through an inferior pericardiotomy[12], and after remission of infection, the patient would be re-evaluated for dual-chamber pacemaker implantation.
For statistical analysis, continuous variables are expressed as mean or median and categorical variables are reported as frequency and percentages. Continuous variables were compared using a two-sample t-test.
The study proposal was approved by the Heidelberg University ethics commission (S-597/2019). All patients in this study consented to use of their medical records for research purposes.
RESULTS
During the 11 years of study period, we performed percutaneous laser lead extractions in 274 patients, of which six patients (1.82%) suffered from axillo-subclavian vein thrombosis. Patient characteristics can be seen in Table 1.
| Patient No. | Age (years)/sex | Indication for CIED | Indication for LLE | Number of extracted leads |
Age of leads (months) | Comorbid conditions |
|---|---|---|---|---|---|---|
| 1 | 73/male | VT | Pocket infection | 4 | 59 | DM, HTN |
| 2 | 68/male | VT and LBBB | Pocket infection | 3 | 95 | DM, HTN |
| 3 | 66/male | VT | Lead perforation | 1 | 146 | HTN, CAD |
| 4 | 62/male | AVB | Painful pocket | 1 | 39 | DM, HTN |
| 5 | 53/female | SSS | Lead endocarditis | 2 | 121 | HTN, CAD |
| 6 | 80/male | SSS | Pocket infection | 2 | 100 | CAD, HTN |
AVB=atrioventricular block; CAD=coronary artery disease; CIED=cardiac implantable electronic devices; DM=diabetes mellitus; HTN=arterial hypertension; LBBB=left bundle branch block; LLE=laser lead extraction; VT=ventricular tachycardia; SSS=sick sinus syndrome

Mean age of the patients was 64±7 years. A total of 11 leads with a mean age of 92±43.8 months were extracted. All leads were completely extracted except in patient No. 1, in whom the double-coil lead was partially removed. Types of extracted leads are listed in Table 2.
| Patient No. | Single-coil lead | Double-coil lead | RV lead | RA lead | LV lead |
|---|---|---|---|---|---|
| 1 | 1 | 1 | 1 | 1 | |
| 2 | 1 | 1 | 1 | ||
| 3 | 1 | ||||
| 4 | 1 | ||||
| 5 | 1 | 1 | |||
| 6 | 1 | 1 |
LV=left ventricular; RA=right atrial; RV=right ventricular

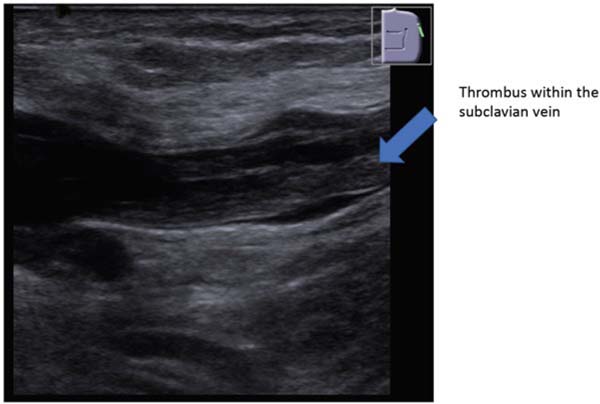
All patients presented with arm swelling and purplish discoloration. Patients No. 1 to 4 had also pain in the affected arms. Patient No. 1, who received bilateral laser lead extraction, developed a superior vena cava syndrome with symptomatic bilateral arm swelling with pain and purplish discoloration and flushing. In patient No.1, computed tomography angiography confirmed the diagnosis and showed bilateral thrombosis of both axillary and subclavian veins and thrombosis of the innominate vein and the superior vena cava. In patients No. 2 and 3, a duplex ultrasound confirmed the thrombosis of axillary and subclavian veins on the side of laser lead extraction (Figure 1). In patient No. 3, the venogram showed preoperative stenosis of the left subclavian vein and postoperative thrombosis of the same subclavian vein. Patient No. 5 developed thrombosis of the subclavian vein, which was confirmed in computed tomography angiography (Figure 2). Patient No. 6 suffered from thrombosis of the left axillary vein after ipsilateral laser lead extraction, which was confirmed by duplex ultrasound.
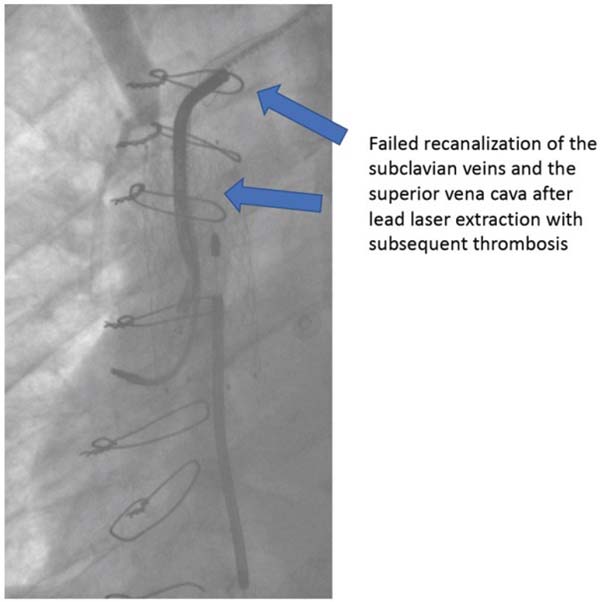
All patients received intravenous unfractionated heparin with elevation of the arm and compression bandage. Because of the severity of the symptoms, patient No. 1 received balloon angioplasty with stent implantation in the superior vena cava and the right subclavian vein. The symptoms diminished but two years later, a new phlebography showed complete rethrombosis of the superior vena cava and a balloon angioplasty was performed with initial success. However, five years later, complete thrombosis of the superior vena cava was detected, and no further intervention was undertaken (Figure 3). Patients No. 2, 3, 4, and 6 were treated medically and received anticoagulation for three months postoperatively. Patient No. 5 was also treated medically and due to worsening of his general condition, he was admitted to the intensive care unit. After developing pneumonia with respiratory failure, patient 5 died 87 days later.
DISCUSSION
The pathogenesis of axillo-subclavian vein thrombosis after percutaneous laser lead extraction is not well understood. The long-lying leads develop adhesions and fibrosis in the venous system making simple removal troublesome. This fibrosis depends on the dwell time of the hardware and young patient age[12]. The use of laser sheaths bears the risk of inducing vessel or organ injury and sometimes embolism of tissue fragments[8,11]. As described by Tarakji et al.[13], the removed leads contain remnants of vascular, atrial, and ventricular tissue, which creates abrasive surfaces in the venous system. The exposure of those surfaces to blood flow may trigger thrombus formation and vein occlusion. Albertini et al.[14] has also detected a significant degree of upper extremity deep venous thrombosis occurring after laser lead extraction, which is often underdiagnosed. In addition, the remnant of partially removed leads, as in patient No.1, may also enhance this thrombotic effect. Also, the number of the extracted leads plays a role in this process as an increase in the number of laser rounds may increase the abraded surface area in the vein making thrombus formation more likely. The use of balloon angioplasty may alleviate the symptoms and gives time for the development of collateral circulation, but central vein patency may not be long-lasting. Generally, unilateral axillo-subclavian thrombosis can be well tolerated, and the symptoms subside over time under the use of anticoagulants with compression bandages and arm elevation, as collateral circulation develops to reduce the congestion. The only permanent problem is that the affected veins in our case series are not available for future lead implantation. Also, axillo-subclavian thrombosis may not cause complete venous occlusion, and in this way, it will be clinically symptomatic. This asymptomatic partial or complete occlusion of the axillo-subclavian vein will make future lead implantation questionable. Fu et al.[15] reported three patients with superior vena cava syndrome after laser lead extraction with subsequent lead implantation. Also, Ghosh et al.[16] reported three cases of venous thrombosis after laser lead extraction. This may raise the question, whether the venous thrombosis was a result of the extraction or the implantation[17] or both. Also, the use of laser lead extraction in a stenosed vein, as in patient No. 3, may increase the chances of postoperative venous thrombosis as the generated tunnel is composed of injured surfaces, which are more amenable to thrombosis.
CONCLUSION
Laser lead extraction may cause symptomatic venous occlusion affecting patients’ quality of life. A larger number of patients with a longer follow-up duration and frequent postoperative testing are needed to identify the patients at risk and to uncover silent venous thrombosis. Intravenous heparin followed by oral anticoagulants and venoplasty of the superior vena cava occlusion should help alleviating the symptoms. Discovering silent thrombosis may alter our approach to laser lead extraction.
REFERENCES
1. Raatikainen MJ, Arnar DO, Merkely B, Camm AJ, Hindricks G. Access to and clinical use of cardiac implantable electronic devices and interventional electrophysiological procedures in the European society of cardiology countries: 2016 report from the European heart rhythm association. Europace. 2016;18 Suppl 3:iii1-iii79. doi:10.1093/europace/euw244. [MedLine]
2. Sohail MR, Uslan DZ, Khan AH, Friedman PA, Hayes DL, Wilson WR, et al. Management and outcome of permanent pacemaker and implantable cardioverter-defibrillator infections. J Am Coll Cardiol. 2007;49(18):1851-9. doi:10.1016/j.jacc.2007.01.072. [MedLine]
3. Goldberger Z, Lampert R. Implantable cardioverter-defibrillators: expanding indications and technologies. JAMA. 2006;295(7):809-18. doi:10.1001/jama.295.7.809. [MedLine]
4. Bongiorni MG, Burri H, Deharo JC, Starck C, Kennergren C, Saghy L, et al. 2018 EHRA expert consensus statement on lead extraction: recommendations on definitions, endpoints, research trial design, and data collection requirements for clinical scientific studies and registries: endorsed by APHRS/HRS/LAHRS. Europace. 2018;20(7):1217. Erratum in: Europace. 2018;20(7):1167. doi:10.1093/europace/euy050.
5. Greenspon AJ, Patel JD, Lau E, Ochoa JA, Frisch DR, Ho RT, et al. Trends in permanent pacemaker implantation in the United States from 1993 to 2009: increasing complexity of patients and procedures. J Am Coll Cardiol. 2012;60(16):1540-5. doi:10.1016/j.jacc.2012.07.017.
6. Love CJ, Wilkoff BL, Byrd CL, Belott PH, Brinker JA, Fearnot NE, et al. Recommendations for extraction of chronically implanted transvenous pacing and defibrillator leads: indications, facilities, training. North American society of pacing and electrophysiology lead extraction conference faculty. Pacing Clin Electrophysiol. 2000;23(4 Pt 1):544-51. doi:10.1111/j.1540-8159.2000.tb00845.x.
7. Novak M, Dvorak P, Kamaryt P, Slana B, Lipoldova J. Autopsy and clinical context in deceased patients with implanted pacemakers and defibrillators: intracardiac findings near their leads and electrodes. Europace. 2009;11(11):1510-6. doi:10.1093/europace/eup216.
8. Bongiorni MG, Kennergren C, Butter C, Deharo JC, Kutarski A, Rinaldi CA, et al. The European lead extraction controlled (ELECTRa) study: a European heart rhythm association (EHRA) registry of transvenous lead extraction outcomes. Eur Heart J. 2017;38(40):2995-3005. doi:10.1093/eurheartj/ehx080.
9. Byrd CL, Wilkoff BL, Love CJ, Sellers TD, Reiser C. Clinical study of the laser sheath for lead extraction: the total experience in the United States. Pacing Clin Electrophysiol. 2002;25(5):804-8. doi:10.1046/j.1460-9592.2002.t01-1-00804.x.
10. Kusumoto FM, Schoenfeld MH, Wilkoff BL, Berul CI, Birgersdotter- Green UM, Carrillo R, et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm. 2017;14(12):e503-51. Erratum in: Heart Rhythm. 2021;18(10):1814. doi:10.1016/j.hrthm.2017.09.001.
11. Wazni O, Epstein LM, Carrillo RG, Love C, Adler SW, Riggio DW, et al. Lead extraction in the contemporary setting: the LExICon study: an observational retrospective study of consecutive laser lead extractions. J Am Coll Cardiol. 2010;55(6):579-86. Erratum in: J Am Coll Cardiol. 2010;55(10):1055. doi:10.1016/j.jacc.2009.08.070.
12. Al-Maisary SSA, Romano G, Karck M, De Simone R. Epicardial pacemaker as a bridge for pacemaker-dependent patients undergoing explantation of infected cardiac implantable electronic devices. J Card Surg. 2019;34(6):424-7. doi:10.1111/jocs.14058.
13. Tarakji KG, Saliba W, Markabawi D, Rodriguez ER, Krauthammer Y, Brunner MP, et al. Unrecognized venous injuries after cardiac implantable electronic device transvenous lead extraction. Heart Rhythm. 2018;15(3):318-25. doi:10.1016/j.hrthm.2017.11.008.
14. Albertini CMM, da Silva KR, Lima MF, Leal Filho JMDM, Martinelli Filho M, Costa R. Upper extremity deep venous thrombosis and pulmonary embolism after transvenous lead replacement or upgrade procedures. Pacing Clin Electrophysiol. 2020;43(5):495-502. doi:10.1111/pace.13915.
15. Fu HX, Huang XM, Zhong L, Osborn MJ, Bjarnason H, Mulpuru S, et al. Outcome and management of pacemaker-induced superior vena cava syndrome. Pacing Clin Electrophysiol. 2014;37(11):1470-6. doi:10.1111/pace.12455.
16. Ghosh N, Yee R, Klein GJ, Quantz M, Novick RJ, Skanes AC, et al. Krahn AD Laser lead extraction: is there a learning curve? Pacing Clin Electrophysiol. 2005;28(3):180-4. doi:10.1111/j.1540-8159.2005.09368.x.
17. Lickfett L, Bitzen A, Arepally A, Nasir K, Wolpert C, Jeong KM, et al. Incidence of venous obstruction following insertion of an implantable cardioverter defibrillator. A study of systematic contrast venography on patients presenting for their first elective ICD generator replacement. Europace. 2004;6(1):25-31. doi:10.1016/j.eupc.2003.09.001.
Authors’Roles & Responsibilities
SAM= Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
JK= Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
GR= Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
MK= Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
RS= Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
Article receive on Friday, September 23, 2022
Article accepted on Saturday, February 4, 2023
 All scientific articles published at rbccv.org are licensed under a Creative Commons license
All scientific articles published at rbccv.org are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()




 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket