![]()
![]()
Aleksandr ZotovI; Daniil BorisovII; Aleksandr TroitskiyI; Robert KhabazovI
DOI: 10.21470/1678-9741-2022-0146
ABSTRACT
Introduction: We propose a new technique for box-lesion ablation combined with off-pump coronary artery bypass grafting for the treatment of patients with coronary artery disease and paroxysmal or persistent atrial fibrillation.AF = Atrial fibrillation
CABG = Coronary artery bypass grafting
CAD = Coronary artery disease
CHA₂DS₂VASc = Congestive heart failure, hypertension, age ≥ 75 (doubled), diabetes, stroke (doubled), vascular disease, age 65 to 74, and sex category (female)
LA = Left atrial
OPCABG = Off-pump coronary artery bypass grafting
PaAF = Paroxysmal atrial fibrillation
PeAF = Persistent atrial fibrillation
PV = Pulmonary vein
INTRODUCTION
Atrial fibrillation (AF) is common in many patients presenting for cardiac surgery[1]. Data from the Society of Thoracic Surgeons indicates that AF is present in 5.1% of patients requiring coronary artery bypass grafting (CABG)[2]. Nevertheless, concomitant ablation was performed in only 33.0% of patients undergoing isolated CABG[2]. The development of technically more convenient techniques used in beating heart surgery may support a wider introduction of AF ablation in CABG patients.
In some patients, beating heart exposure of pulmonary veins (PVs) results in haemodynamic instability and that is why we offer to use a flexible ablation device (Cardioblate™ Gemini™-S). This device is widely used in thoracoscopic procedures with promising mid- and long-term results[3-5].
METHODS
Study Population
From August till December 2019, eight male patients underwent surgical off-pump revascularization with concomitant box-lesion ablation and left atrial (LA) appendage resection. All patients had symptomatic coronary artery disease (CAD) and paroxysmal (PaAF) or persistent atrial fibrillation (PeAF). No other cardiac surgical procedure was performed.
Patients’ baseline characteristics are summarized in Table 1.
| Male, n (%) | 8 (100%) |
| Paroxysmal atrial fibrillation, n (%) | 2 (25%) |
| Persistent atrial fibrillation, n (%) | 6 (75%) |
| Age, years, median (min-max) | 67 (59; 75) |
| CHA₂DS₂VASc, median (min-max) | 2 (1; 4) |
| Duration of atrial fibrillation, months, median (min-max) | 26 (5; 42) |
| Previous history of acute myocardial infarction, n (%) | 6 (75%) |
| Previous history of thromboembolic events, n (%) | 2 (25%) |
| Stroke | 1 |
| Transient ischemic attack | 1 |
| Body mass index, kg/m2, median (min-max) | 30 (24; 35) |
| Left atrial diameter, mm, median (min-max) | 43 (35; 49) |
| Indexed left atrial volume, ml/m2, median (min-max) | 55 (42; 67) |
| Left ventricular ejection fraction, Simpson, %, median (min-max) | 50 (42; 63) |
| Pulmonary artery pressure, mmHg, median (min-max) | 36 (24; 52) |
| Hypertension, n (%) | 6 (75%) |
| Chronic obstructive pulmonary disease, n (%) | 2 (25%) |
| Diabetes, n (%) | 3 (37.5%) |
| Glomerular filtration rate < 60 mL/min/1.73 m2, n (%) | 2 (25%) |
CHA₂DS₂VASc=congestive heart failure, hypertension, age ≥ 75 (doubled), diabetes, stroke (doubled), vascular disease, age 65 to 74, and sex category (female)

The study protocol was approved by the Local Ethics Committee (P19/0021), and all patients signed informed consent forms prior to surgery.
Surgical Procedure
After median sternotomy, the conduits were harvested, and heparin was administered. Left internal mammary artery and saphenous vein were used as grafts.
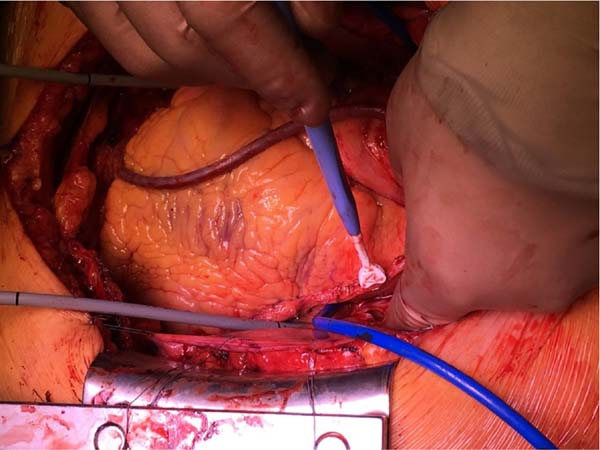
Coronary revascularization was performed before ablation using tissue stabilizers and apical suction positioning devices. Proximal anastomoses were performed using Heartstring® Proximal Seal System. On completion of grafts, intraoperative graft flows were assessed using a flowmeter (Figure 1).
The ablation was performed using a flexible bipolar irrigated ablation device - Cardioblate™ Gemini™-S. The device was designed for thoracoscopic procedures as was described by Doty et al.[3] in the original paper.
Blunt dissection was performed to open the transverse sinus by entering the space between the right pulmonary artery and the right superior PV (posterior to the junction of the superior vena cava and right atrium). The oblique sinus (the space between the right inferior PV and the inferior vena cava) was opened in the same fashion.
Two rubber catheters were passed through the sinuses behind the left atrium, above and below the superior and inferior PVs to guide the device clamps (Figure 1). The clamps were then attached to ends of the catheters outside the wound.
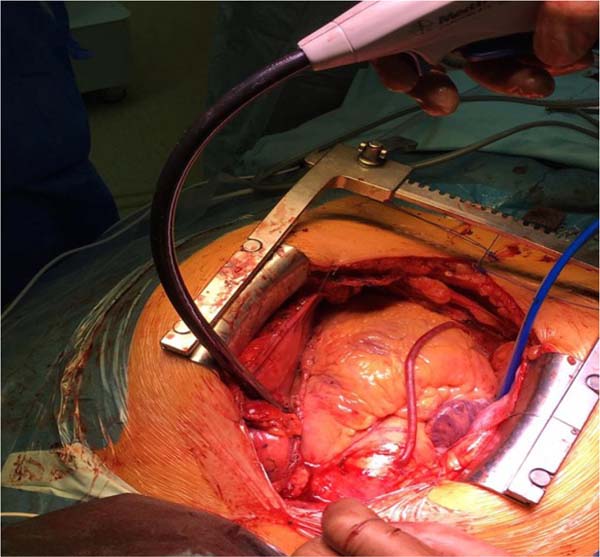
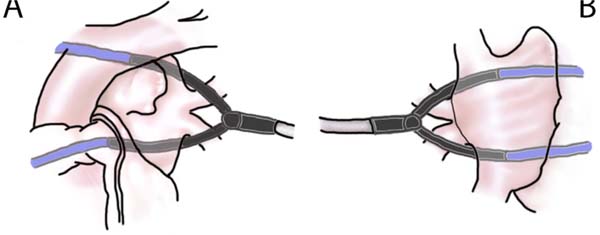
Gentle traction on ends of the catheters was used to draw the device into position across left PVs and left atrium. Once appropriately positioned, it was clamped over the left half of the left atrium (Figures 2, 3A). Ten lesions were applied guided by impedance drop to confirm transmurality. After each application, the device was adjusted a little to get overlapping lesions. The process was then repeated on the right side - hereby creating a box lesion (Figure 3B).
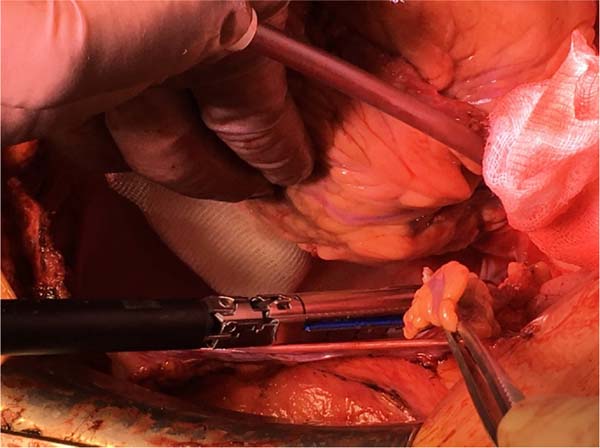
The LA appendage was resected with an Echelon™ or Endo GIA™ stapler (Figure 4).
Afterwards, electrical cardioversion was used to restore sinus rhythm and bilateral epicardial stimulation was performed to check the block of conduction. Exit block was confirmed by pacing the PVs and nonablated tissue within the box after cardioversion with a maximum output of 25 mA. In case of ventricular capture, additional ablation was performed until exit block could be confirmed.
Postoperative Management and Follow-up
Statins, antihypertensive drugs (if required), and bisoprolol were taken routinely after surgery. Amiodarone was administered intravenously before extubation, and this was followed by amiodarone taken orally for a period of six months. If a patient was in sinus rhythm and symptoms free, antiarrhythmic drugs were stopped after six months. Low-molecular-weight heparin was administered at a prophylactic dose, starting the day after the procedure until the day of discharge. Afterwards, low-molecular-weight heparin was replaced with dabigatran.
All patients were monitored continuously for arrhythmias in intensive care unit. Twenty-four-hour Holter monitoring and transthoracic echocardiography were performed at three, six, and 12 months postoperatively. Recurrence was defined as any electrocardiographically documented episode of AF, atrial flutter, or atrial tachycardia lasting > 30 seconds occurring beyond a three-month blanking period. Patients were encouraged to contact a doctor in case of symptoms of AF or previously unrecognized symptoms. Stress echocardiography was performed at 12 months to confirm freedom from CAD.
Generally, dabigatran was discontinued after six months in the absence of atrial tachyarrhythmia recurrences unless prior thromboembolism or other indication for chronic anticoagulation.
RESULTS
There was no operative mortality, no myocardial infarction, and no stroke nor transient ischemic attack. Two patients with PaAF were in sinus rhythm before the procedure. Electrical cardioversion on the operating table was successful in four patients with PeAF. Conduction block was confirmed in all patients with sinus rhythm.
Detailed periprocedural data and complications are shown in Table 2.
| Surgery time, minutes, median (min; max) | 190 (142; 247) |
| Ablation time, minutes, median (min; max) | 18 (16; 23) |
| Number of grafts per patient, median (min; max) | 3 (2; 4) |
| Left atrial appendage resection, n (%) | 8 (100%) |
| Intubation time, hours, median (min; max) | 5 (4; 8) |
| Time with chest tubes, hours, median (min; max) | 24 (14; 70) |
| Postoperative blood loss, ml, median (min; max) | 350 (250; 750) |
| Intensive care unit stay, hours, median (min; max) | 18 (14; 32) |
| Hospital stay, days, median (min; max) | 8 (5; 14) |
| Complications, n (%) | 2 |
| Need for blood product transfusion | 1 |
| Pleural effusion requiring drainage | 1 |

In two patients with PeAF, sinus rhythm was restored within 24 hours, after amiodarone infusion and electrical cardioversion. AF recurred on postoperative day four in one patient, and the sinus rhythm was restored after electrical cardioversion.
All patients underwent a control examination three, six, and 12 months after the procedure.
At a median follow-up of 14 months (range 12-17), there were no signs of recurrence of AF nor other supraventricular arrhythmia in seven patients (87.5%). AF recurred in one patient who had long-standing PeAF before the surgery. The form of AF in this patient shifted to paroxysmal. Therefore, amiodarone was used for rhythm control.
Stress echocardiography at 12 months showed freedom from CAD in all patients.
DISCUSSION
This is the first study showing safety and feasibility of box-lesion ablation with the use of a flexible clamping device during off-pump CABG (OPCABG).
Previous studies have shown that surgical ablation of AF concomitant with bypass surgery provides improved long-term survival[6]. In randomized controlled trials and matched patient populations, surgical ablation of AF during cardiac surgery proved to be safe, effective at restoring sinus rhythm, and associated with late improved exercise capacity and survival compared to untreated patients[2,6].
The recent guidelines gave Class I recommendations for the concomitant surgical ablation of AF without additional risk of operative mortality or major morbidity[7,8]. They recommended surgical AF ablation at the time of concomitant CABG (Level B) to restore sinus rhythm[7,8]. Although the Cox-Maze procedure remains the gold standard for surgical treatment of AF, the necessity of performing a Maze procedure for all AF patients is a debatable issue. The downside of such procedure is opening of the left atrium for ablation which requires cardiopulmonary bypass. In those patients who do undergo surgical AF ablation, the most commonly performed ablation procedure is PV isolation, simply because of technical difficulties when faced to do more[9]. Technical issues can be encountered in patients with a low left ventricular ejection fraction or an enlarged heart, as these patients may not tolerate the procedure hemodynamically. OPCABG is already a challenging procedure in such patients, and further manipulating the heart during ablation and pacing may be problematic.
Intraoperative hypoperfusion may result in organ ischemic damage and increase the risk of postoperative complications such as stroke or acute renal insufficiency[10]. The use of flexible ablation device helps to overcome these difficulties.
We believe that the described technique can be successfully combined with conventional on-pump CABG and minimally invasive CABG (in this scenario some steps of ablation procedure are performed thoracoscopically). Importantly, the use of this technique does not require intensive training and high level of surgical skills.
At the same time, we need to admit that box-lesion ablation cannot be effectively used in patients with pulmonary artery hypertension (pulmonary artery pressure > 45 mmHg), prolonged history of AF (> 5 years), prominent LA dilatation (indexed LA volume > 48 ml/m2), or significant mitral valve disease. In these groups of patients, concomitant Cox-Maze IV procedure would be preferrable.
REFERENCES
1. McCarthy PM, Davidson CJ, Kruse J, Lerner DJ, Braid-Forbes MJ,McCrea MM, et al. Prevalence of atrial fibrillation before cardiac surgery andfactors associated with concomitant ablation. J Thorac Cardiovasc Surg.2020;159(6):2245-53.e15. doi:10.1016/j.jtcvs.2019.06.062.
2. Badhwar V, Rankin JS, Ad N, Grau-Sepulveda M, Damiano RJ, GillinovAM, et al. Surgical ablation of atrial fibrillation in the United States: trendsand propensity matched outcomes. Ann Thorac Surg. 2017;104(2):493-500.doi:10.1016/j.athoracsur.2017.05.016. [MedLine]
3. Doty JR, Clayson SE. Surgical treatment of isolated (lone) atrialfibrillation with gemini-S ablation and left atrial appendage excision (GALAXYprocedure). Innovations (Phila). 2012;7(1):33-8.doi:10.1097/IMI.0b013e3182560612. [MedLine]
4. Guo QZ, Zhu D, Bai ZX, Shi J, Shi YK, Guo YQ. A novel "boxlesion" minimally invasive totally thoracoscopic surgical ablation foratrial fibrillation. Ann Acad Med Singap. 2015;44(1):6-12. [MedLine]
5. Janusauskas V, Puodziukaite L, Maneikiene VV, Zuoziene G, Radauskaite G, Burneikaite G, et al. Long-term results of minimally invasive stand-alone bi-atrial surgical ablation with a bipolar ablation device for persistent and longstanding persistent AF: a singlecenter case series of 91 patients. J Cardiothorac Surg. 2016;11:23. doi:10.1186/s13019-016-0416-0.
6. Musharbash FN, Schill MR, Sinn LA, Schuessler RB, Maniar HS, Moon MR, et al. Performance of the cox-maze IV procedure is associated with improved long-term survival in patients with atrial fibrillation undergoing cardiac surgery. J Thorac Cardiovasc Surg. 2018;155(1):159-70. doi:10.1016/j.jtcvs.2017.09.095.
7. Badhwar V, Rankin JS, Damiano RJ Jr, Gillinov AM, Bakaeen FG, Edgerton JR, et al. The society of thoracic surgeons 2017 clinical practice guidelines for the surgical treatment of atrial fibrillation. Ann Thorac Surg. 2017;103(1):329-41. doi:10.1016/j.athoracsur.2016.10.076.
8. Ad N, Damiano RJ Jr, Badhwar V, Calkins H, La Meir M, Nitta T, et al. Expert consensus guidelines: examining surgical ablation for atrial fibrillation. J Thorac Cardiovasc Surg. 2017;153(6):1330-54.e1. doi:10.1016/j.jtcvs.2017.02.027.
9. Khiabani AJ, Adademir T, Schuessler RB, Melby SJ, Moon MR, Damiano RJ Jr. Management of atrial fibrillation in patients undergoing coronary artery bypass grafting: review of the literature. Innovations (Phila). 2018;13(6):383-90. doi:10.1097/IMI.0000000000000570.
10. O'Neal JB, Shaw AD, Billings FT 4th. Acute kidney injury following cardiac surgery: current understanding and future directions. Crit Care. 2016;20(1):187. doi:10.1186/s13054-016-1352-z
Authors’Roles & Responsibilities
AZ= Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
DB= Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
AT= Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
RK= Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
Article receive on Wednesday, March 30, 2022
Article accepted on Monday, September 5, 2022
 All scientific articles published at rbccv.org are licensed under a Creative Commons license
All scientific articles published at rbccv.org are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()




 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket