![]()
![]()
Abdullah DemirhanI; Yusuf VelioğluII; Hamit YoldasI; Ibrahim KaragozI; Mehmet CosgunIII; Duygu CaliskanI; Isa YildizI; Murat BilgiI; Kemalettin ErdemII
DOI: 10.21470/1678-9741-2018-0282
ABSTRACT
Objective: To investigate the effects of preoperative anxiety relieving on electrophysiological changes in patients undergoing off-pump coronary artery bypass surgery.ASA = American Society of Anesthesiologists
BAI = Beck Anxiety Inventory
BMI = Body mass index
DBP = Diastolic blood pressure
ECG = Electrocardiography
HR = Heart rate
HT = Heart transplantation
MAP = Mean arterial pressure
QTc = Corrected QT interval
Pd = P-wave dispersion
PO = Per os
QTc = Corrected QT
QTd = QT dispersion
SBP = Systolic blood pressure
SPSS = Statistical Package for Social Science
STAI-I = State Trait Anxiety Inventory
TI = Tracheal intubation
INTRODUCTION
Major cardiac surgery causes fear, stress and anxiety on many patients[1-5]. Due to concern, fear and due to some unknown reasons, it is stated that patients may experience high levels of anxiety prior to cardiac surgery[6]. It has been previously shown that one or two days before cardiac surgery the anxiety levels of patients rises up to 20-50%[2,3].
Anxiety, depression and negative thoughts may also cause pathological changes[7]. It has been found that increased anxiety leads to sympathetic hyperactivity through elevated levels of serotonin, dopamine, plasma norepinephrine and metabolites in patients[8,9]. This, in return, decreases the ventricular fibrillation threshold via prolonged and increased dispersion of repolarization[10]. It has been shown in the literature that increased anxiety and stress levels may increase the likelihood of cardiac arrhythmia through prolonged QT dispersion (QTd)[11,12].
It is known that coronary bypass surgery causes more catecholamine release during laryngoscopy and tracheal intubation (TI) compared to other operations, resulting in a sudden increase in blood pressure and heart rate (HR)[13,14]. Previous studies have also shown that increased plasma levels of catecholamine increase P-wave dispersion (Pd) on electrocardiography, prolong corrected QT (QTc) distance, and QT dispersion. Moreover, Pd changes have been associated with atrial arrhythmias, however, changes in QTc and QTd were associated with ventricular arrhythmia and sudden death[15-17].
Electrocardiography (ECG) is a reliable indicator that is frequently used to detect pathological electrical activity. The QT interval is an indicative of ventricular repolarization, and its extension is considered a risk factor for arrhythmias[18]. QT dispersion is defined as the difference between the longest QT and the shortest QT of the 12-lead ECG reflecting the different regions of ventricular repolarization. Laryngoscopy and TI in anesthesia induction increases HR and mean arterial pressure (MAP) values, as well as changes the electrophysiological properties of the heart[19-23]. In the literature, inhalers have been shown to extend QT interval following anesthetic agents and TI[24,25].
In this study, we investigated the effects of relieving preoperative anxiety on electrophysiological changes in patients who will undergo off-pump coronary artery bypass surgery. In these patients, high levels of stress are induced during pre-induction, as well as laryngoscopy and tracheal intubation.
METHODS
The present randomized controlled study was performed after approval of the Abant Izzet Baysal University Ethics Committee for Clinical Researches by 2017/05. All patients provided their written and oral consent to participate in the study during preoperative examination. All patients underwent off-pump coronary artery bypass grafting surgery under general anesthesia, performed in Abant Izzet Baysal University at the Training Research Hospital. A total of 61 patients in ASA III risk group in the age range of 18-65 years were enrolled in the present study. Sixty-one patients, who agreed to participate in the study, were randomly divided into two groups. The group administered with anxiolytic-sedative drug was called Group S (Sedation group), and the group that was not administered any anxiolytic-sedative drug was called Group C (Control group). Group S was administered 0.04 mg/kg lorazepam per os (PO) twice; once the night before the operation, then 2 hours before the operation. Group C was not administered with any anxiolytic premedication.
Evaluations were performed and recorded using both the State Trait Anxiety Inventory-TX1 (STAI-I) form, consisting of 20 parameters, and the Beck Anxiety Inventory (BAI), consisting of 21 parameters for the state anxiety measurement of the patients. STAI-I is used to show the individual differences in anxiety levels, which is intensified in response to potentially threatening events[26]. In this questionnaire, a total score of 20 to 80 was given to each participant using a 4-point Likert scale. In this test, higher scores are indicative of elevated anxiety levels[26-28]. BAI was scored from 0 to 3 using a 4-point Likert scale. This test is used to focus on somatic symptoms of anxiety[29].
On the day of operation, the STAI-I and BAI evaluations were performed by a practitioner who did not know the patient's groups. In the operating room, 16-18 G intravenous catheters were inserted into separate arms and 0.05 mg/kg morphine was administered intravenously to provide sedation. For all patients, ECG for heart rate (HR), pulse oximetry (SpO2) for peripheral oxygen saturation and standard monitoring were performed. Moreover, to monitor the arterial blood pressure, Allen test was performed from a normal arm under topical anesthesia using a 20G catheter. The systolic blood pressure (SBP), diastolic blood pressure (DBP) and MAP parameters were also recorded. Furthermore, during preanesthetic induction, patients were connected with standard 12-lead ECG (Nihon Kohden, Model EKG-1350K, Japan) to confirm sinus rhythm and pre-induction ECG recording was obtained. ECG recordings were performed at a speed of 25 mm/sec.
Anesthesia induction was started using 1-2 mg/kg propofol and 2 mcg/kg fentanyl. After loss of consciousness, muscle relaxation was achieved with 0.6 mg/kg rocuronium. This is followed by face mask ventilation for 3 minutes. Then, patients were intubated using a tube of similar size (size 8). Following the 12-lead ECG induction of the patients, after induction at the 1st and 3rd minutes, as well as after intubation, at the 30th second in the 2nd and 4th minutes, records were taken. Then, the anesthesia was continued with air and 1-2% sevoflurane in 50% oxygen. At the same time, central venous catheter was inserted, and hemodynamic parameters, including HR and MAP, were measured and recorded before induction, after induction at the 1st and 3rd minutes, as well as after intubation and at the 30th second in the 2nd and 4th minutes. QT and P dispersion in each derivation of all ECGs was calculated by a cardiologist and anesthesiologist. The QT dispersion was calculated as the difference between the maximum and minimum QT values (QTd = maximum QT - minimum QT). Likewise, P dispersion was calculated as the difference between the maximum and minimum P-values.
Statistical Analysis
The Statistical Package for Social Science (SPSS 23.0) program was used to perform statistical analysis. The descriptive variables age, body mass index (BMI), QT dispersion, P dispersion, and MAP were calculated as mean ± standard deviation. The Kolmogorov-Smirnov test was used to determine whether variables were normally distributed. Independent-Samples T-test was used to analyze the normally distributed variables between the groups. Analysis of variance for repeated measures was used to compare QT dispersion, P dispersion and MAP at different intubation time periods. When a significant overall effect was detected, Tukey’s post-hoc test was conducted for comparison of the mean values for the two variables. The chi-squared and Fisher's exact tests were used for the analysis of the categorical variables. A P-value less than 0.05 (P<0.05) was considered as the statistical significance limit. Compared with previous studies[30], to achieve α<0.05 and β=80% according to QT dispersion, 22 subjects were required in the control group, and 22 subjects were required in the sedation group.
RESULTS
There was no significant difference between groups in terms of age, gender, BMI and duration of intubation (P>0.05) (Table 1). Preoperative STAI-I scores were significantly lower in sedation group compared to the controls (P<0.05) (Table 2). When BAI and STAI scores were compared within the group, no significant difference was observed in Group S (P=0.102). However, the scores were significantly higher in Group C (P<0.001) (Table 2).
| Characteristic | Group S (n=30) | Group C (n=31) | P -value |
|---|---|---|---|
| Age (years) | 63.4±8.6 | 60.5±11.2 | 0.272 |
| Body mass index (kg/m2) | 28.3±3.6 | 27.1±3.2 | 0.159 |
| Male, N (%) | 25 (83.3%) | 27 (87.1%) | 0.731 |
| Female, N (%) | 5 (16.7%) | 4 (12.9%) | |
| Duration of intubation (sec) | 9.3±3.3 | 8.3±2.1 | 0.180 |
| Mean number of grafts | 4.0±0.9 | 3.7±1.3 | 0.274 |

| Group S | Group C | |||||||
|---|---|---|---|---|---|---|---|---|
| BAI | STAI | BAI | STAI | |||||
| Preoperative | 4.8±4.5 | P =0.102 | 35.0±9.6 | P =0.031 | 5.9±7.4 * | P <0.001 | 41.4±10.4 * | P <0.001 |
| Before induction | 3.3±4.7 | 31.1±9.5 | 10.2±8.7 * | 51.6±11.1 * | ||||
* Indicates statistical significance.

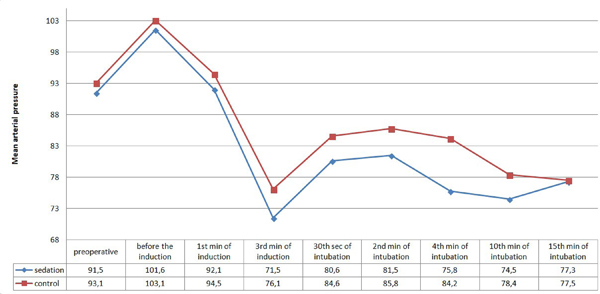
In the intergroup evaluation of the cases, MAP values during intraoperative period showed no significant difference (P>0.05) (Figure 1). Heart rate was only significantly reduced in Group S following the 30th second of intubation (Figure 2).
The differences between these groups were examined by multiple comparison tests. According to these results, mean values of QTd measured before induction, at the 1st minute of induction, 30th second of intubation and 4th minute of intubation in sedation group were significantly reduced compared to controls (P=0.024; P=0.027; P=0.001; P=0.033, respectively) (Table 3).
| QT dispersion (msec) | Group S | Group C | P -value |
|---|---|---|---|
| Preoperative | 46.0 (±8.7) | 46.7 (±7.4) | 0.734 |
| Before induction | 46.9 (±9.6) | 51.9 (±6.8) | 0.024 * |
| 1st min of induction | 46.4 (±7.9) | 50.1 (±4.3) | 0.027 * |
| 3rd min of induction | 48.0 (±6.7) | 47.5 (±5.4) | 0.727 |
| 30th sec of intubation | 50.7 (±6.8) | 55.9 (±4.9) | 0.001 * |
| 2nd min of intubation | 48.6 (±6.0) | 51.5 (±6.0) | 0.068 |
* There was a statistically significant difference between Group C and Group S ( P <0.05).

The mean values of P dispersion measured before induction, at the 3rd minute of induction, 30th second of intubation and 4th minute of intubation in sedation group were significantly reduced compared to the controls (P=0.001; P=0.020; P=0.023; P=0.005, respectively) (Table 4).
| P dispersion (msec) | Group S | Group C | P -value |
|---|---|---|---|
| Preoperative | 31.2 (±3.1) | 31.8 (±3.4) | 0.447 |
| Before induction | 30.4 (±3.9) | 33.9 (±3.9) | 0.001 * |
| 1st min of induction | 31.0 (±2.2) | 31.9 (±3.2) | 0.232 |
| 3rd min of induction | 30.4 (±2.2) | 32.7 (±4.8) | 0.020 * |
| 30th sec of intubation | 38.2 (±3.1) | 40.1 (±3.1) | 0.023 * |
| 2nd min of intubation | 34.3 (±3.1) | 35.9 (±2.9) | 0.051 |
| 4th min of intubation | 32.2 (±2.4) | 34.0 (±2.3) | 0.005 * |
* There was a statistically significant difference between Group C and Group S ( P <0.05).

DISCUSSION
The current study showed that the high anxiety levels of patients who underwent coronary bypass surgery had increased QTd and Pd intervals. On the other hand, removal of preoperative anxiety shortened QTd and Pd intervals in pre-induction and following laryngoscopy and TI procedures.
The main reasons of increased level of preoperative anxiety in cardiac surgeries in patients awaiting coronary artery bypass surgery are unawareness of surgery and the fear caused by the lack of knowledge. It is considered normal for intense anxiety in patients a couple of days before the surgery or during the surgery preparations. Lichtor et al.[31] reported that the anxiety level of the patient during the day before surgery was not different from the level of anxiety prior to entering the operating room in the day of surgery. Some of the patients experienced high levels of anxiety and this increased levels has been associated with increased QT dispersion leading to cardiac arrhythmias[11]. It has also been shown that mental stress can increase QT dispersion[12]. In the present study, we observed that BAI and STAI scores of anxiety-deprived patients, who were waiting for coronary bypass surgery, showed a decrease in preoperative turnover compared to preoperative turnout, where BAI and STAI scores were increased in the control group. The results of the present study suggest that increased anxiety assessment scores in the control group increased patients’ preoperative anxiety. As a result, it significantly increased QTd and Pd intervals before induction. The results of the current study for the effects of anxiety on QTd and Pd were similar to those previously published in the literature[11,12]. Due to the prolonged QT dispersion leading to ventricular arrhythmias and the risk of sudden death[32,33], we have shown that it is important to reduce patients’ anxiety levels before surgery.
In the literature, the effect of implementation of laryngoscopy, a procedure that prolongs the QTD and Pd interval, and TI[15-17,30] in QT or P dispersions in a patient undergoing anxiety-relieved coronary bypass surgery has not been reported. Catecholamine release and stress response during laryngoscopy and TI can lead to severe complications in patients with cardiovascular and cerebral disease, as well as increase the risk of mortality and morbidity[15,34]. It has been reported that QT dispersion could be used for HT patients as an indicator for the prevention of sudden cardiac death[35,36]. In addition, the QTd interval after TI is prolonged and is even more severe in patients with coronary artery disease and HT[21]. Similar to the QT dispersion, prolonged Pd interval is considered to be indicative of supraventricular arrhythmias. In many studies, Pd interval has been reported to be a useful and simple method for determining the risk of paroxysmal atrial fibrillation[37]. Changes in the P-wave interval in patients with diastolic dysfunction, myocardial ischaemia and acute coronary syndrome have been shown in the literature[38,39]. Previous studies have shown that volatile anesthetics and TI may prolong the QT interval period[24]. On the other hand, the use of propofol, as an intravenous anesthetics, may be more appropriate without prolonging the QT interval[40] and shortens the Pd interval[41]. Likewise, administration of fentanyl at a dose of 2 mcg/kg before induction of propofol has been shown to reduce the length of laryngoscopy and TI-dependent QTc interval[42]. In the current study, we also used drugs with positive effects on laryngoscopy and QT and P dispersion durations during TI. Moreover, we also observed that propofol and fentanyl decreased laryngoscopy and TI-dependent QT and P dispersions. We found that the elimination of anxiety contributed more positive effects to decrease the QT and Pd times. In the literature, although it has been reported that some benzodiazepines may lead to alterations on electrocardiographic parametres[43,44], there are several studies reporting that lorazepam does not directly affect electrocardiographic parametres. including PR prolongation, QRS widening and QTc interval[45-47]. Therefore, we designed this study on the preference of lorazepam as anxiolytic agent.
In conclusion, the results of the present study demonstrate that high anxiety levels in patients with coronary artery disease and coronary bypass surgery have a negative effect through prolonged QT and Pd times. Moreover, anxiety removal before surgery may be useful to prevent ventricular and atrial arrhythmias and associated complications by decreasing the QT and P-wave dispersion durations both during pre-induction and the peak periods of stress response due to laryngoscopy and tracheal intubation.
REFERENCES
1. Lindsay GM, Smith LN, Hanlon P, Wheatley DJ. Coronary artery diseasepatients' perception of their health and expectations of benefitfollowing coronary artery bypass grafting. J Adv Nurs. 2000;32(6):1412-21.doi:10.1046/j.1365-2648.2000.01621.x.
2. Rymaszewska J, Kiejna A, Hadrys T. Depression and anxiety incoronary artery bypass grafting patients. Eur Psychiatry. 2003;18(4):155-60.doi:10.1016/S0924-9338(03)00052-X.
3. Krannich JH, Weyers P, Lueger S, Herzog M, Bohrer T, Elert O.Presence of depression and anxiety before and after coronary artery bypass graftsurgery and their relationship to age. BMC Psychiatry. 2007;7:47.doi:10.1186/1471-244X-7-47.
4. Yuksel V, Gorgulu Y, Cinar RK, Huseyin S, Sonmez MB, Canbaz S.Impact of experiencing acute coronary syndrome prior to open heart surgery onpsychiatric status. Braz J Cardiovasc Surg. 2016;31(4):281-6.doi:10.5935/1678-9741.20160064. [MedLine]
5. Garbossa A, Maldaner E, Mortari DM, Biasi J, Leguisamo CP. Effectsof physiotherapeutic instructions on anxiety of CABG patients. Rev Bras CirCardiovasc. 2009;24(3):359-66.doi:10.1590/S0102-76382009000400016.
6. Fitzsimons D, Parahoo K, Stringer M. Waiting for coronary arterybypass surgery: a qualitative analysis. J Adv Nurs. 2000;32(5):1243-52.doi:10.1046/j.1365-2648.2000.01595.x.
7. Hemingway H, Marmot M. Evidence based cardiology: psychosocialfactors in the aetiology and prognosis of coronary heart disease. Systematicreview of prospective cohort studies. BMJ . 1999 ;318(7196):1460-7. Available from:
8. Argyropoulos SV, Bell CJ, Nutt DJ. Brain function in social anxietydisorder. Psychiatr Clin North Am. 2001;24(4):707-22.doi:10.1016/S0193-953X(05)70259-8.
9. Sevy S, Papadimitriou GN, Surmont DW, Goldman S, Mendlewicz J.Noradrenergic function in generalized anxiety disorder, major depressivedisorder, and healthy subjects. Biol Psychiatry. 1989;25(2):141-52.doi:10.1016/0006-3223(89)90158-3.
10. Schwartz PJ. Idiopathic long QT syndrome: progress and questions. AmHeart J. 1985;109(2):399-411. doi:10.1016/0002-8703(85)90626-X. [MedLine]
11. Kelmanson IA. High anxiety in clinically healthy patients andincreased QT dispersion: a meta-analysis. Eur J Prev Cardiol.2014;21(12):1568-74. doi:10.1177/2047487313501613.
12. Hassan M, Mela A, Li Q, Brumback B, Fillingim RB, Conti JB, et al.The effect of acute psychological stress on QT dispersion in patients withcoronary artery disease. Pacing Clin Electrophysiol. 2009;32(9):1178-83.doi:10.1111/j.1540-8159.2009.02462.x.
13. Shribman AJ, Smith G, Achola KJ. Cardiovascular and catecholamineresponses to laryngoscopy with and without tracheal intubation. Br J Anaesth.1987;59(3):295-9. doi:10.1093/bja/59.3.295.
14. Russell WJ, Morris RG, Frewin DB, Drew SE. Changes in plasmacatecholamine concentrations during endotracheal intubation. Br J Anaesth.1981;53(8):837-9. doi:10.1093/bja/53.8.837.
15. Le Heuzey JY, Guize L. Cardiac prognosis in hypertensive patients.Incidence of sudden death and ventricular arrhythmias. Am J Med.1988;84(1B):65-8. doi:10.1016/S0002-9343(88)91161-8.
16. Ormaetxe JM, Martinez Alday JD, Almendral J, Alfageme Beobide M,Iriarte M. Prognostic significance of ventricular arrhythmias in the presence ofpathological left ventricular hypertrophy. Eur Heart J . 1993 ;14 Suppl J:73-5. Available from:
17. Zareba W, Moss AJ, le Cessie S. Dispersion of ventricularrepolarization and arrhythmic cardiac death in coronary artery disease. Am JCardiol. 1994;74(6):550-3. doi:10.1016/0002-9149(94)90742-0.
18. Roden DM. Acquired long QT syndromes and the risk of proarrhythmia.J Cardiovasc Electrophysiol. 2000;11(8):938-40.doi:10.1111/j.1540-8167.2000.tb00077.x.
19. Hanci V, Yurtlu S, Karabag T, Okyay D, Hakimoglu S, Kayhan G, et al.Effects of esmolol, lidocaine and fentanyl on P wave dispersion, QT, QTcintervals and hemodynamic responses to endotracheal intubation during propofolinduction: a comparative study. Braz J Anesthesiol. 2013;63(3):235-44.doi:10.1016/S0034-7094(13)70223-X.
20. Hanci V, Aydin M, Yurtlu BS, Ayoglu H, Okyay RD, Tas E, et al.Anesthesia induction with sevoflurane and propofol: evaluation of P-wavedispersion, QT and corrected QT intervals. Kaohsiung J Med Sci.2010;26(9):470-7. doi:10.1016/S1607-551X(10)70074-7.
21. Ay B, Fak AS, Toprak A, Gogus YF, Oktay A. QT dispersion increasesduring intubation in patients with coronary artery disease. J Electrocardiol.2003;36(2):99-104. doi:10.1054/jelc.2003.50017. [MedLine]
22. Erdil F, Demirbilek S, Begec Z, Ozturk E, But A, Ozcan Ersoy M. Theeffect of esmolol on the QTc interval during induction of anaesthesia inpatients with coronary artery disease. Anaesthesia. 2009;64(3):246-50.doi:10.1111/j.1365-2044.2008.05754.x.
23. Cafiero T, Di Minno RM, Di Iorio C. QT interval and QT dispersionduring the induction of anesthesia and tracheal intubation: a comparison ofremifentanil and fentanyl. Minerva Anestesiol. 2011;77(2):160-5.doi:10.1097/00003643-200606001-00134.
24. Schmeling WT, Warltier DC, McDonald DJ, Madsen KE, Atlee JL, KampineJP. Prolongation of the QT interval by enflurane, isoflurane, and halothane inhumans. Anesth Analg. 1991;72(2):137-44.doi:10.1213/00000539-199102000-00001.
25. Kuenszberg E, Loeckinger A, Kleinsasser A, Lindner KH, Puehringer F,Hoermann C. Sevoflurane progressively prolongs the QT interval in unpremedicatedfemale adults. Eur J Anaesthesiol. 2000;17(11):662-4.doi:10.1046/j.1365-2346.2000.00739.x.
26. Barnes LL, Harp D, Jung WS. Reliability generalization of scores onthe Spielberger state-trait anxiety inventory. Educational and PsychologicalMeasurement. 2002;62(4):603-18.doi:10.1177/0013164402062004005.
27. Kok L, Sep MS, Veldhuijzen DS, Cornelisse S, Nierich AP, van derMaaten J, et al. Trait anxiety mediates the effect of stress exposure onpost-traumatic stress disorder and depression risk in cardiac surgery patients.J Affect Disord. 2016;206:216-23.doi:10.1016/j.jad.2016.07.020. [MedLine]
28. Kvaal K, Ulstein I, Nordhus IH, Engedal K. The SpielbergerState-Trait Anxiety Inventory (STAI): the state scale in detecting mentaldisorders in geriatric patients. Int J Geriatr Psychiatry. 2005;20(7):629-34.doi:10.1002/gps.1330.
29. Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuringclinical anxiety: psychometric properties. J Consult Clin Psychol.1988;56(6):893-7. doi:10.1037/0022-006X.56.6.893.
30. Kiraci G, Demirhan A, Tekelioglu UY, Akkaya A, Bilgi M, Erdem A, etal. A comparison of the effects of lidocaine or magnesium sulfate on hemodynamicresponse and QT dispersion related with intubation in patients withhypertension. Acta Anaesthesiol Belg . 2014 ;65(3):81-6. Available from:
31. Lichtor JL, Johanson CE, Mhoon D, Faure EA, Hassan SZ, Roizen MF.Preoperative anxiety: does anxiety level the afternoon before surgery predictanxiety level just before surgery? Anesthesiology . 1987 ;67(4):595-9. Available from:
32. Glancy JM, Garratt CJ, Woods KL, de Bono DP. QT dispersion andmortality after myocardial infarction. Lancet. 1995;345(8955):945-8.doi:10.1016/S0140-6736(95)90697-5.
33. Buja G, Miorelli M, Turrini P, Melacini P, Nava A. Comparison of QTdispersion in hypertrophic cardiomyopathy between patients with and withoutventricular arrhythmias and sudden death. Am J Cardiol. 1993;72(12):973-6.doi:10.1016/0002-9149(93)91118-2.
34. Kovac AL. Controlling the hemodynamic response to laryngoscopy andendotracheal intubation. J Clin Anesth. 1996;8(1):63-79.doi:10.1016/0952-8180(95)00147-6. [MedLine]
35. Sani IM, Solomon DS, Imhogene OA, Ahmad AM, Bala GS. QT dispersionin adult hypertensives. J Natl Med Assoc . 2006 ;98(4):631-6. Available from:
36. Clarkson PB, Naas AA, McMahon A, MacLeod C, Struthers AD, MacDonaldTM. QT dispersion in essential hypertension. QJM. 1995;88(5):327-32.doi:10.1093/oxfordjournals.qjmed.a069073.
37. Chang CM, Lee SH, Lu MJ, Lin CH, Chao HH, Cheng JJ, et al. The roleof P wave in prediction of atrial fibrillation after coronary artery surgery.Int J Cardiol. 1999;68(3):303-8.doi:10.1016/S0167-5273(98)00301-5.
38. Gunduz H, Binak E, Arinc H, Akdemir R, Ozhan H, Tamer A, et al. Therelationship between P wave dispersion and diastolic dysfunction. Tex Heart InstJ . 2005 ;32(2):163-7. Available from:
39. Myrianthefs MM, Shandling AH, Startt-Selvester RH, Bernstein SB,Crump R, Lorenz LM, et al. Analysis of the signal-averaged P-wave duration inpatients with percutaneous coronary angioplasty-induced myocardial ischemia. AmJ Cardiol. 1992;70(7):728-32. doi:10.1016/0002-9149(92)90549-E.
40. Erdil F, Demirbilek S, Begec Z, Ozturk E, Ersoy MO. Effects ofpropofol or etomidate on QT interval during electroconvulsive therapy. J ECT.2009;25(3):174-7. doi:10.1097/YCT.0b013e3181903fa5.
41. Owczuk R, Wujtewicz MA, Sawicka W, Polak-Krzeminska A,Suszynska-Mosiewicz A, Raczynska K, et al. Effect of anaesthetic agents onp-wave dispersion on the electrocardiogram: comparison of propofol anddesflurane. Clin Exp Pharmacol Physiol. 2008;35(9):1071-6.doi:10.1111/j.1440-1681.2008.04963.x.
42. Chang DJ, Kweon TD, Nam SB, Lee JS, Shin CS, Park CH, et al. Effectsof fentanyl pretreatment on the QTc interval during propofol induction.Anaesthesia. 2008;63(10):1056-60.doi:10.1111/j.1365-2044.2008.05559.x.
43. Kazemzadeh N, Mohammadi S, Emamhadi M, Amirfarhangi A, Sanaei-ZadehH. Electrocardiographic Manifestations of Benzodiazepine Toxicity. IranianJournal of Toxicology Volume . 2014 ;7(23):952-5.Available from:
44. Ziegenbein M, Kropp S. Lorazepam-induced prolongation of the QTinterval in a patient with schizoaffective disorder and complete AV block. Can JPsychiatry. 2004;49(6):414. doi:10.1177/070674370404900619.
45. Crockford D. Re: Lorazepam-induced prolongation of the QT intervalin a patient with schizoaffective disorder and complete AV block. Can JPsychiatry. 2005;50(3):184-5; author reply 5.doi:10.1177/070674370505000315.
46. Harvey AT, Flockhart D, Gorski JC, Greenblatt DJ, Burke M, Werder S,et al. Intramuscular haloperidol or lorazepam and QT intervals in schizophrenia.J Clin Pharmacol. 2004;44(10):1173-84.doi:10.1177/0091270004267807.
47. Reilly JG, Ayis SA, Ferrier IN, Jones SJ, Thomas SH. QTc-intervalabnormalities and psychotropic drug therapy in psychiatric patients. Lancet.2000;355(9209):1048-52. doi:10.1016/S0140-6736(00)02035-3.
No financial support.
No conflict of interest.
Authors' roles & responsibilities
AD Contribution to the design of the study; data collection; statistical analysis; discussion of results; manuscript writing; article review; final approval of the version to be published
YV Contribution to the design of the study; final approval of the version to be published
HY Data collection; statistical analysis; final approval of the version to be published
IK Data collection; final approval of the version to be published
MC Article review; final approval of the version to be published
DC Article review; final approval of the version to be published
IY Analysis, or interpretation of data for the study; final approval of the version to be published
MB Conception and design of the project; data collection; final approval of the version to be published
KE Data collection; article review; final approval of the version to be published
Article receive on Wednesday, September 12, 2018
Article accepted on Sunday, November 4, 2018
 All scientific articles published at rbccv.org are licensed under a Creative Commons license
All scientific articles published at rbccv.org are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()



 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket